Interesting Cases: GI Series Synchronous rectal and prostate cancer
- 80 Year old gentlemen, Smoker, DM/type2 and Interstitial lung disease
- Presented with 5 month history of stool incontinence, bleeding per rectal and pain while passing stool.
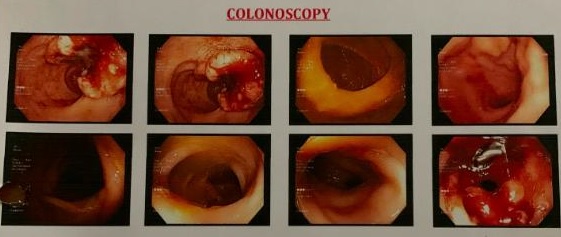
- Sigmoidoscopy showed an ulcerated mass lesion in rectum 5 cm from anal verge
- Biopsy- Adenocarcinoma
After discussion in multispeciality tumour board we decided to treat this patient with 5 weeks of concurrent chemoradiotherapy (CTRT). She received weekly Injection Cisplatin 35 mg/m2 along with 45 Gy/25 Fractions of radiation therapy to cervix, uterus and pelvic lymph nodes with image guided Intensity Modulated Radiation Therapy (IG- IMRT).
Patient tolerated CTRT well and clinically had 80% regression in cervical mass. Repeat MRI at completion of CTRT also showed 80 disease regression with small residual diseases with bilateral medial parametrium infiltration.
The patient was next taken up for Interstitial Brachytherapy along with intra uterine tube placement under USG guidance. USG helped us navigate our needles and tubes in correct position despite multiple large obstructing intrauterine fibroids. This whole procedure was done under spinal anesthesia with epidural catheter for maintain analgesia. Patient with stood this procedure well.
MRI
- MRI Pelvis- growth in distal rectum from 10 to 5’o clock position over length of 4.6cm located above medial attachment of levator ani. Lesion showed marked restriction with mild post contrast enhancement.
- Prostate too showed an incidentally detected T2 hypointense signal measuring 16.6 x 9 mm restricted to right lobe in apex and middle lobe (PIRADS V).
- PSA was 5.7 ng/ml
- Case was discussed meticulously in tumor Board
Tumor board discussion and treatment challenges
- TRUS guided prostate biopsy had high chances of tumor bleed because of another tumor in rectum
- Patient had synchronous adeno carcinoma rectum T3N1M0 and Carcinoma Prostate (T1N0M0)
- Tumour Board decided to treat patient with curative radiation therapy with IGRT technique for both prostate and rectal cancer
- Radiation was given daily to rectal disease and lymph node draining nodal stations as well to the prostate over 5 weeks with simultaneously integrated boost (Higher dose) to prostatic lesion. Patient completed radiation without any significant toxicity.
Tumor board discussion and treatment challenges
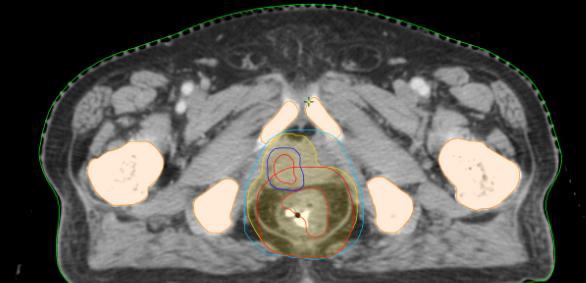
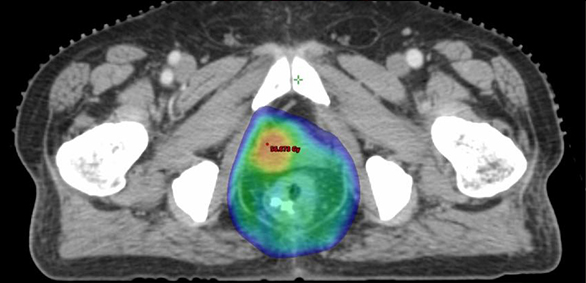
Target involved the prostatic and rectal cancer
Prostate lesion and rectum were included , prostate getting higher dose than rectum
Follow up at 1 year after treatment
- Patient did not undergo surgery and was kept on “watch and wait” protocol with close follow up
- Patient’s bowel bladder habits are normal and totally asymptomatic
- PET Scan and Sigmoidoscopy at 3 months and 1 year of follow up suggested complete metabolic response and no evidence of disease anywhere in body
- PSA <0.4 ng/ml at 1 year
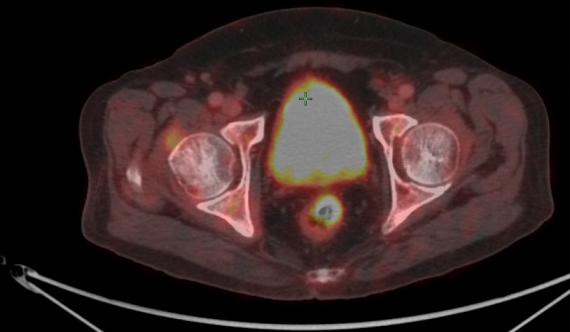
PET CT after 1 year
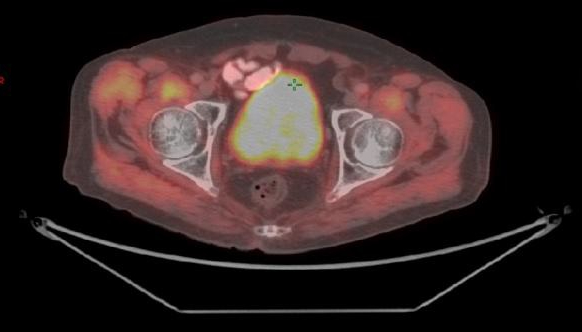
PET CT at Baseline
Take Home Message
- Non surgical treatment for rectal cancer is possible in selected patients
- Informed decision making and compliance are important
- Meticulous tumor board discussion and decision making helps
- Advanced and precise radiation treatment on most modern equipment
- Image Guidance and daily cone beam CT before treatment for exact matching
- Least Possible toxicity to adjacent organs